Foundations
Introduction, medical terminology, palpation skills, and the body’s common postural patterns.
Introduction
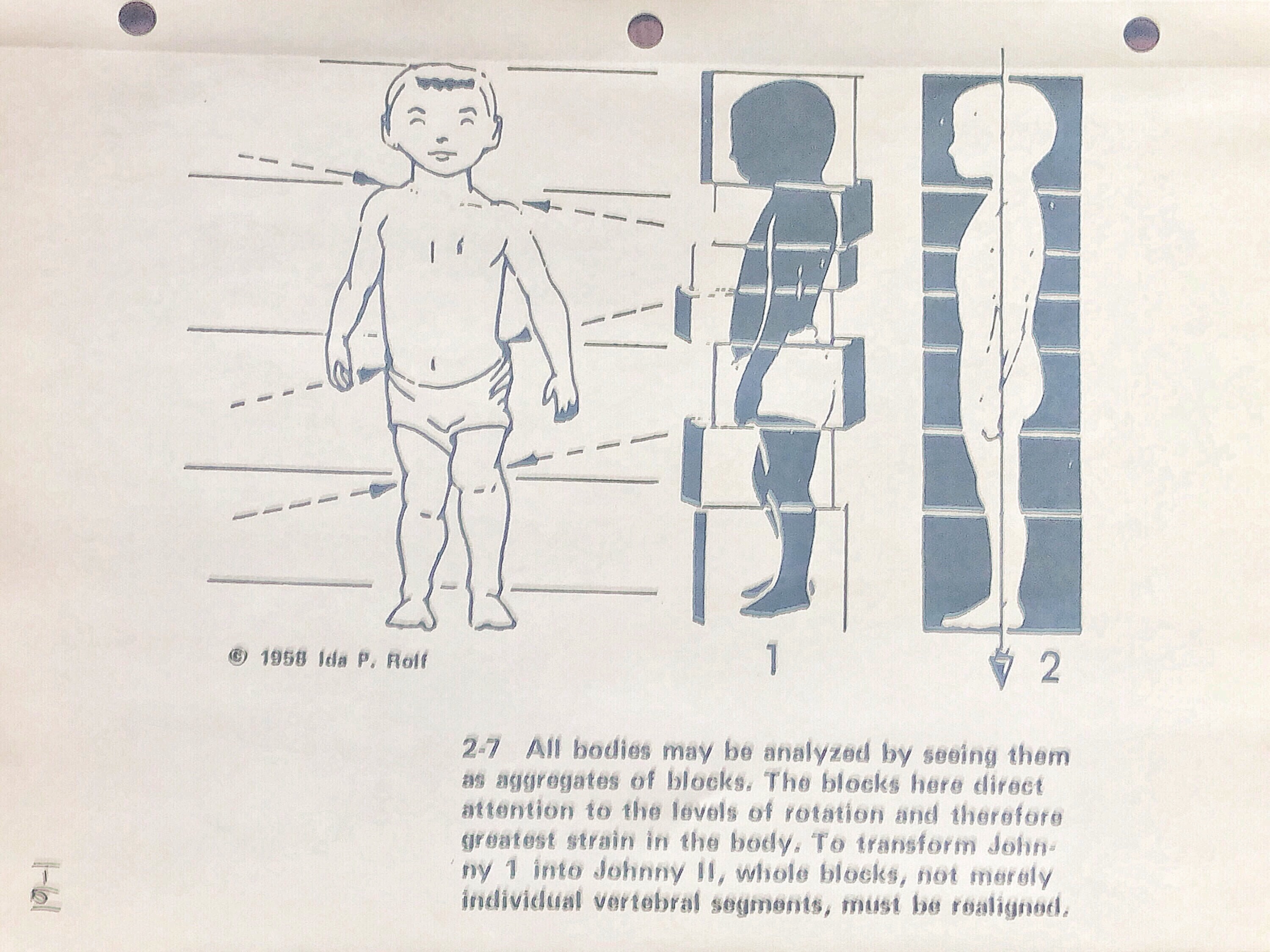
The human body is in a constant state of regeneration. Every tissue continuously rebuilds itself, reinforcing whatever patterns of movement and posture you repeat most often. The body's goal in this process is efficiency — making habitual movements easier by requiring less energy over time.
However, when joints are not moved through their full range of motion, fascial restrictions begin to form. With consistent patterning, even in adulthood, you can change the direction and shape of your skeletal structure. A classic historical example: Victorian women who wore corsets for years developed permanently altered rib cage shapes.
Your thoughts alone carry significant potential to alter your physical state. There are documented cases of individuals with dissociative identity disorder where different identities exhibit different eyesight prescriptions — and even scar tissue that shifts in real time between identities. With deep mind-body practice, people have demonstrated the ability to consciously modulate autonomic nervous system functions, including changing the temperature of individual limbs at will. Your mental projection of your body is highly relevant to your physical experience.
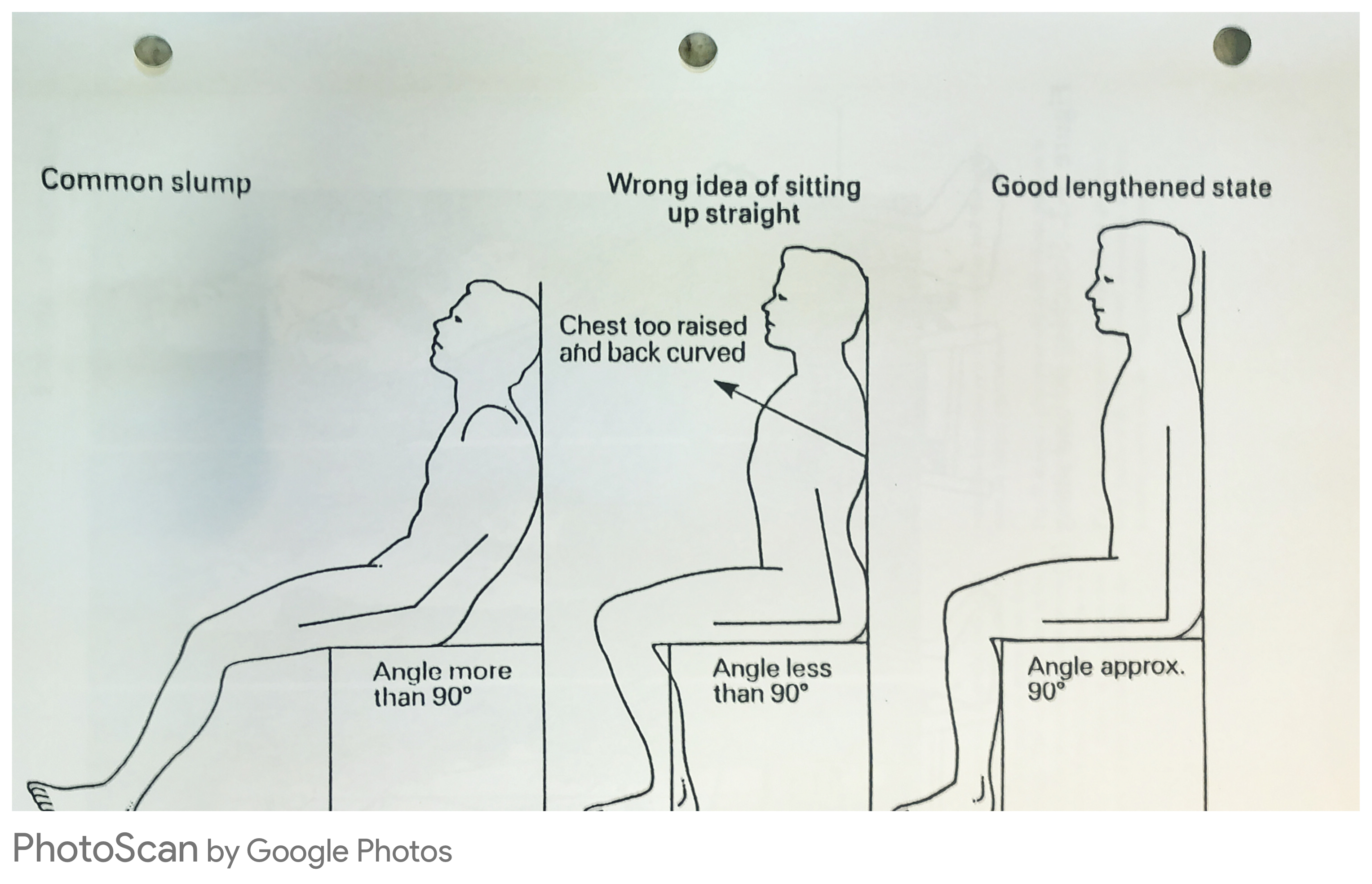
Fortunately, for most people, that level of mastery is not necessary. This manual offers a practical overview of the body's most common postural patterns in the context of modern life, and shows you how to work effectively toward expansion and functional alignment.
Most of your joints are surrounded by a fluid-filled sac called a bursa, which cushions and lubricates movement. When joints are held in compression and fail to express their full range of motion, this synovial fluid can be pushed out of the sac — gradually leading to bone-on-bone contact.
Structural Modalities
Structural approaches — including GOTA, NeuroMuscular Therapy, Rolfing, Osteopathy, Yoga, and Pilates — all confirm and reinforce the same expansive, aligned positioning. The techniques in this manual show how you can achieve meaningful results without prior therapeutic training, using only your hands and two inexpensive tools.
.png)
Theracane — A curved cane-shaped tool that allows you to apply leverage and directed pressure to hard-to-reach areas of your back and hips without straining your hands.
Lacrosse Ball — A firm rubber ball ideal for sustained deep pressure on muscles and fascia, especially when used with body weight.
You don't need to know every muscle to be effective. This manual focuses on what is most clinically relevant. For some techniques I'll outline a series of sequential moves; as your body opens up, you may find it more efficient to skip to the later steps. Through experimentation with body positions and pressure angles, you may also discover modifications that work better for your body.

Medical Terminology
These directional terms are used throughout the manual for anatomical precision. All directions refer to the body in its standard anatomical position — standing upright, palms facing forward.
- Superior
- Toward the head / upward
- Inferior
- Toward the feet / downward
- Anterior
- Toward the front of the body
- Posterior
- Toward the back of the body
- Medial
- Toward the midline of the body
- Lateral
- Away from the midline of the body
- Proximal
- Closer to the point of attachment / trunk
- Distal
- Farther from the point of attachment / trunk
- Fascia
- Connective tissue that surrounds and binds muscles, organs, and structures
- Bursa
- Fluid-filled sac that cushions joints and reduces friction
- Trigger Point
- A hyperirritable spot in muscle tissue that causes localized pain and/or referred pain
- NMT
- NeuroMuscular Trigger point — a trigger point that causes referred pain to distant sites


Palpation Skills
Fascia behaves like a non-Newtonian fluid: to truly access and move it — especially deep fascia — you must move very slowly. Every structure in the body is composed of multiple layers, each with variable tension, density, and sensitivity. You must work through the superficial layers before you can access the deeper ones.
The Art of Sinking In
When making contact with skin, always begin with a soft, slow touch. Use the center of the finger pads for maximum contact and feedback. Once you make contact, gradually sink in rather than push.
Sinking uses your entire body weight and gravity — not local muscle force. The goal is to sink slowly enough that the tissue doesn't push you back out, while simultaneously going deep enough to reach the threshold where resistance meets release. At this threshold, the tissue will begin to let go.
A release commonly feels like the tissue swelling up under your contact, then becoming wide and thin as it lets go. This may take time to feel at first. When you are hitting the right spots with the lacrosse ball, Theracane, fingers, or percussion device, the interaction of tension and release will become much easier to recognize.
A Note on Sensitivity
A common phenomenon: clients present with extremely thick fascia, both superficial and deep. Thick fascia sits further from muscle attachments and nerve endings, which means it registers less sensation. You may feel the urge to press harder because you don't feel much. Resist this impulse.
Instead, slow down, maintain sustained contact, and target the specific points described in each section. Release will come — and over time you'll begin to recognize it clearly.
Palpation Tips by Tool
Use the center of the pads. Sink slowly using body weight, not force. Best for precise work on smaller areas: face, neck, ribs, tendon attachments.
Place between the body and a surface (floor or wall). Use body weight to compress. Excellent for glutes, upper back, thighs, and low back.
Provides leverage to reach the back and hips without straining. Use the rounded hook end for most back work; the pointed end for more targeted depth.
Useful for stimulating circulation and loosening superficial tissue. Use on the abdomen (clockwise) and larger muscle groups before deeper work.
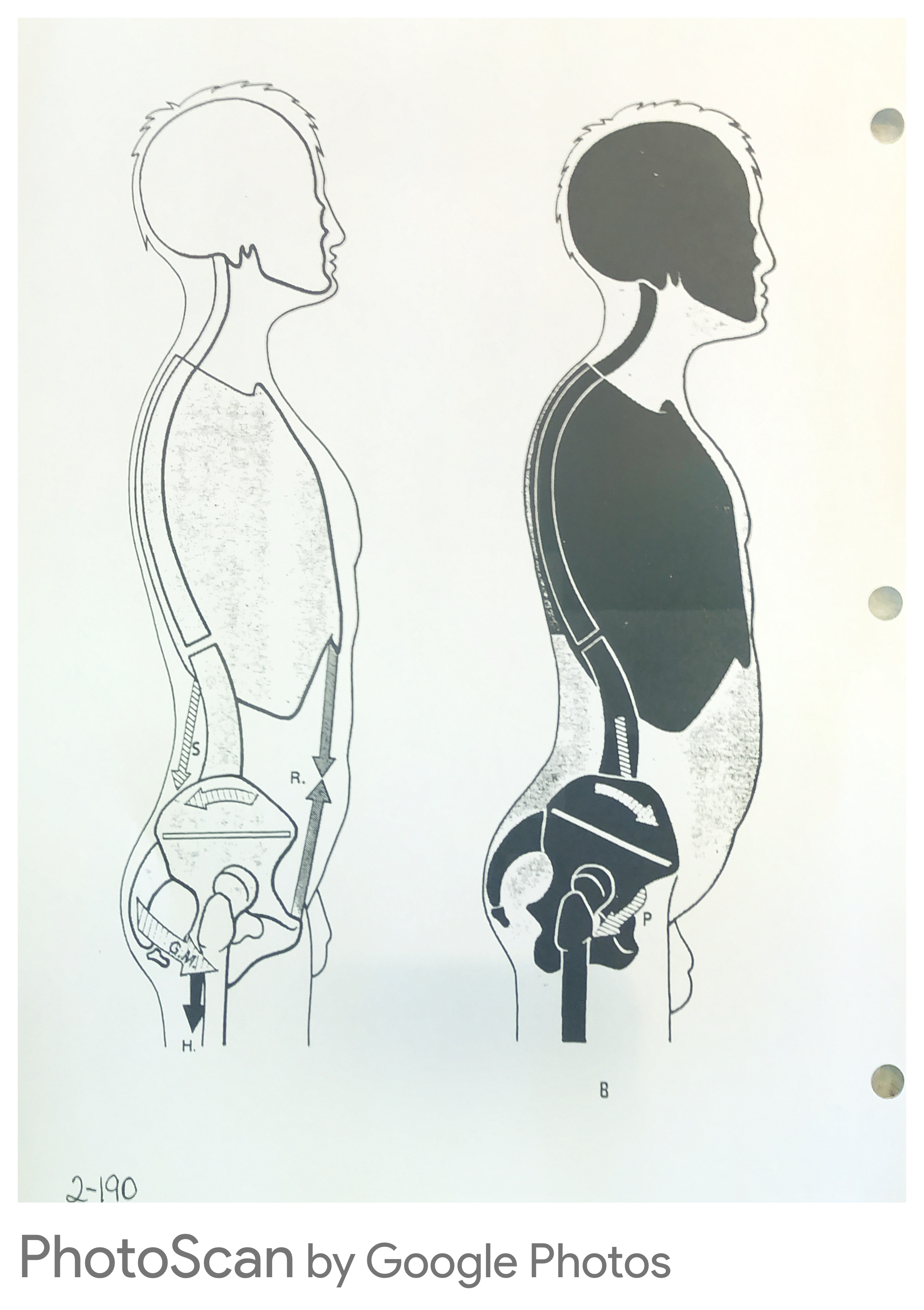
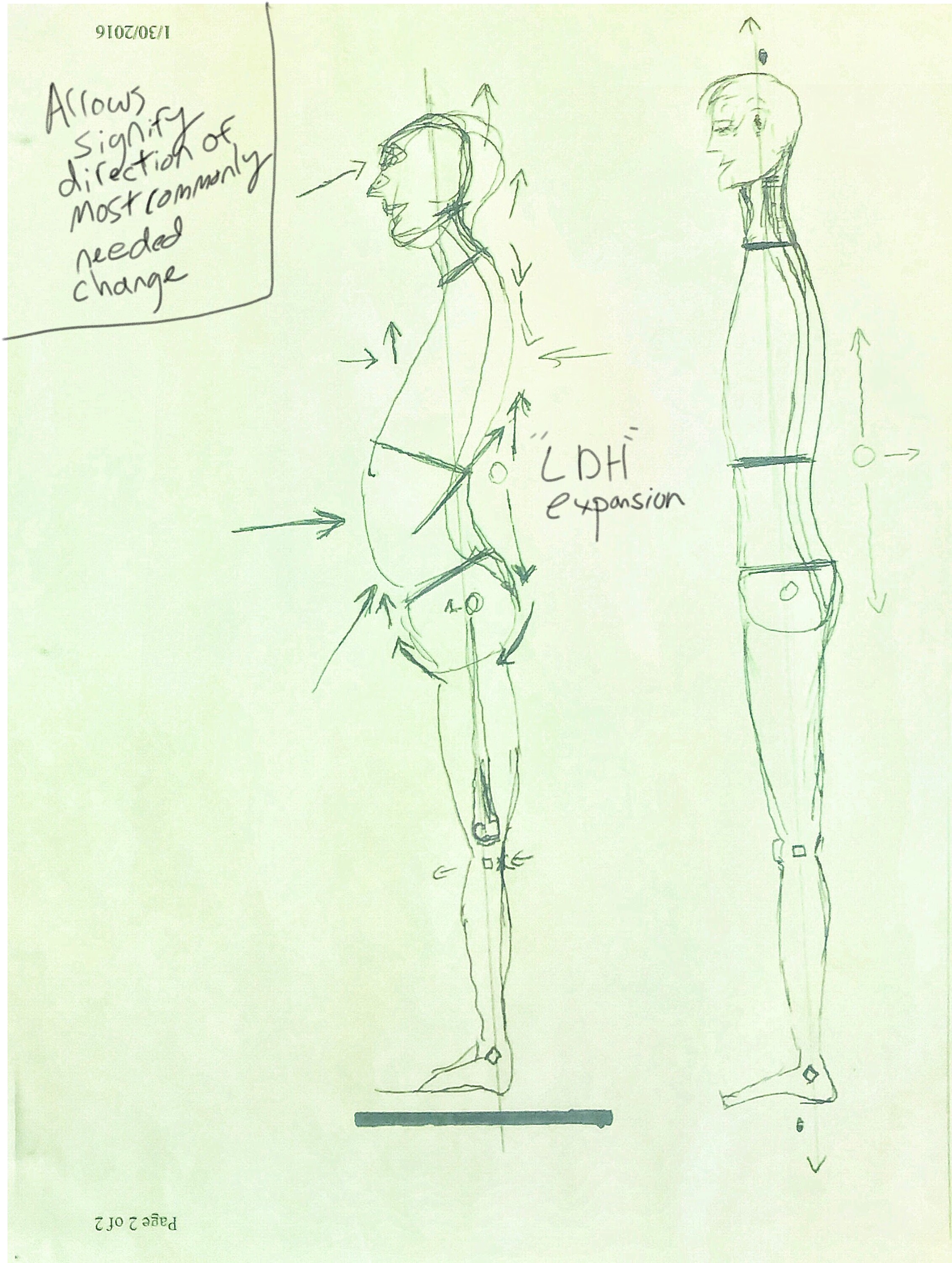
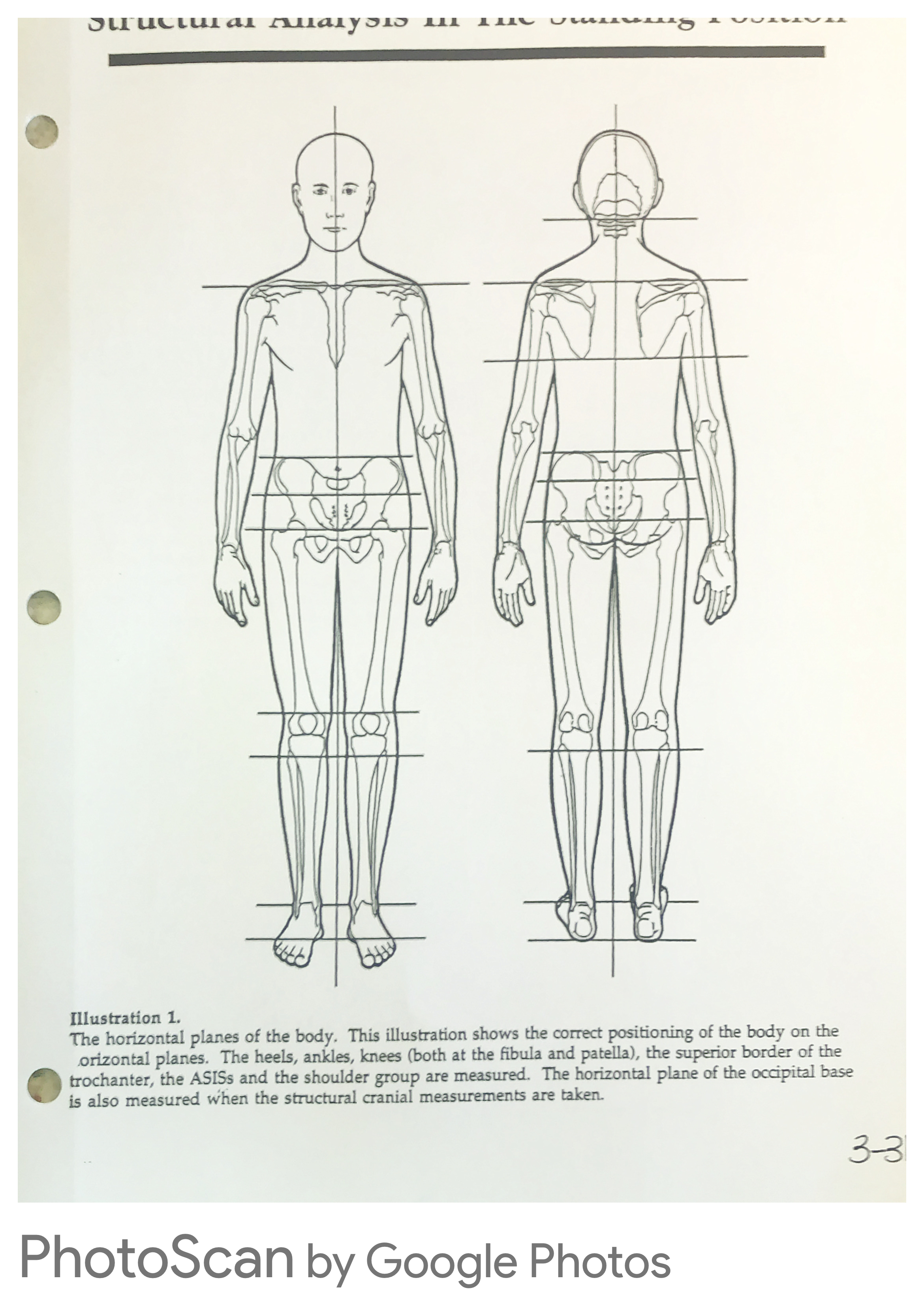
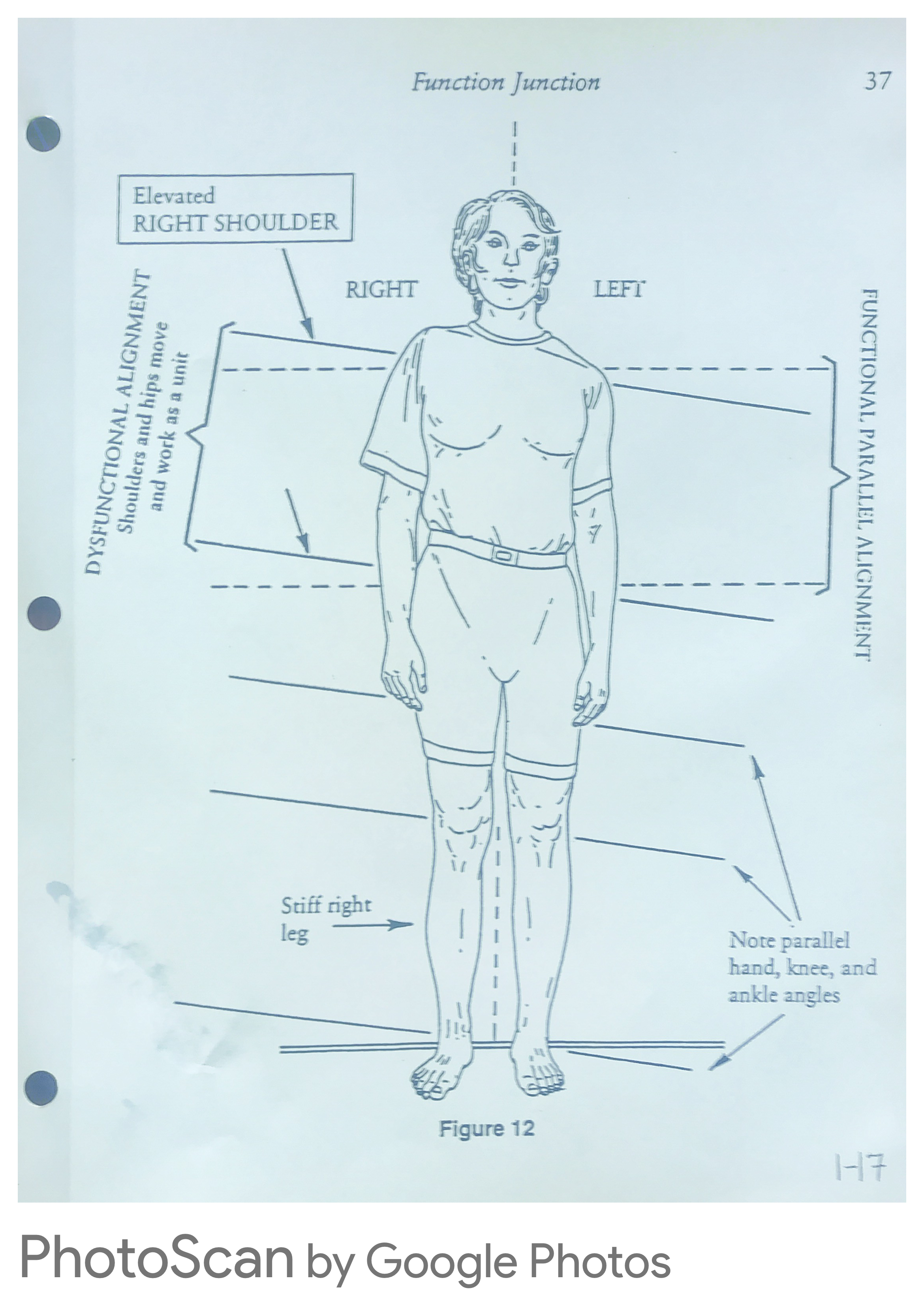
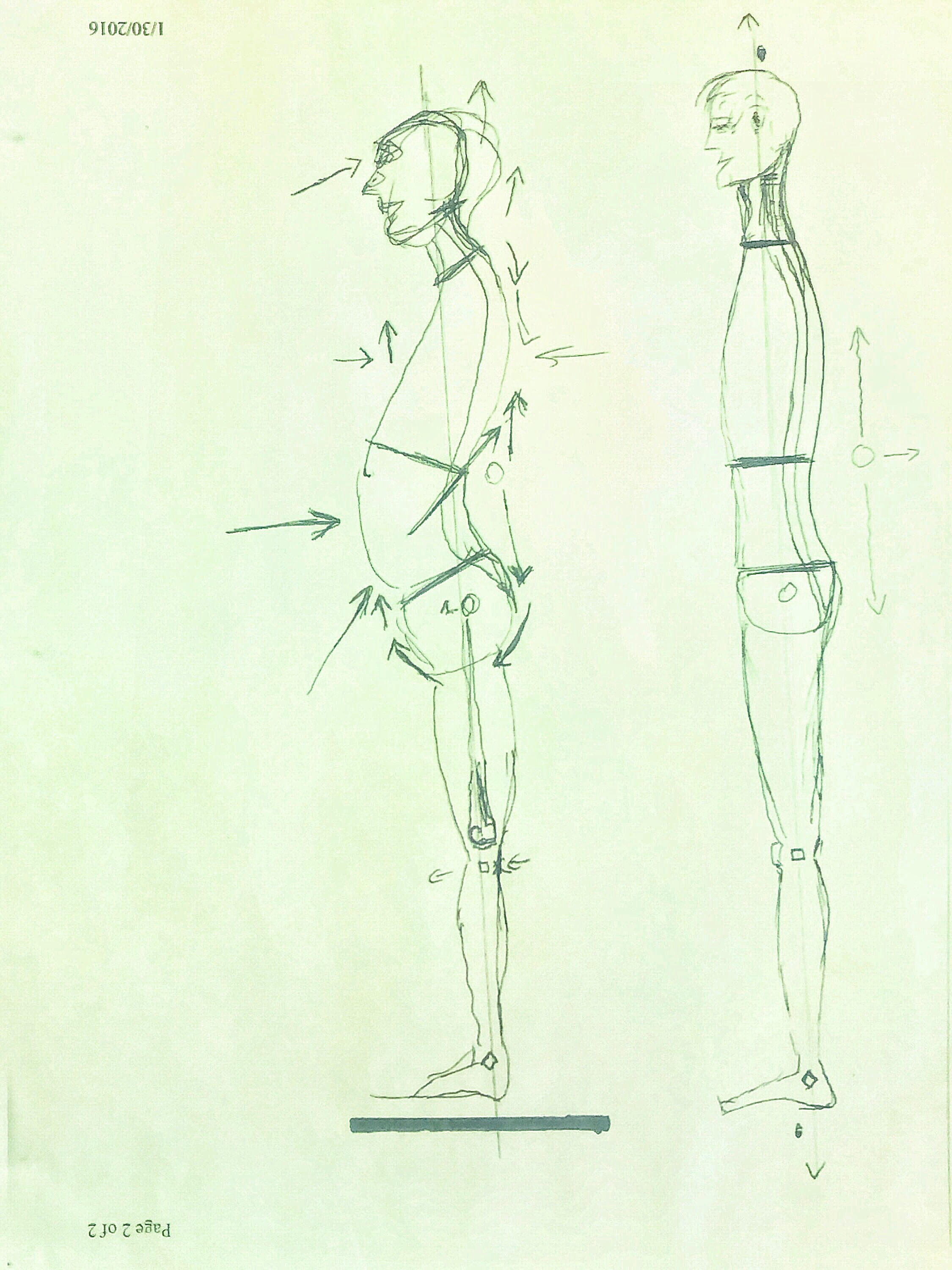
Common Postural Patterns
Modern life — sitting, driving, typing, looking down at screens — produces predictable compressive patterns in the body. Understanding these patterns as a whole helps you see how each region relates to the others. Releasing one area almost always creates ease in adjacent regions.
Feet
Medial (inner) arch collapse; pronation; toes rotated inward; fifth ray supinated.
Legs
External rotation of the entire leg column; Tibia and Fibula compressed together; weak abductors and external rotators.
Hips
Anterior pelvic tilt; sacral compression; weak abdominals; tight, externally rotated psoas; tight glutes.
Thoracic / Mid Back
Lumbodorsal Hinge (LDH) compression; erectors pulled to midline; flared anterior ribs.
Shoulders
Internal rotation of the humerus; shortened pectorals; scapula pulled superior and lateral; weakened external rotators.
Neck & Head
Forward Head Posture (FHP); jaw pushed forward; weak anterior neck muscles; fascial build-up at occiput.


.png)
.png)
.png)
.png)
.png)
.png)
.png)